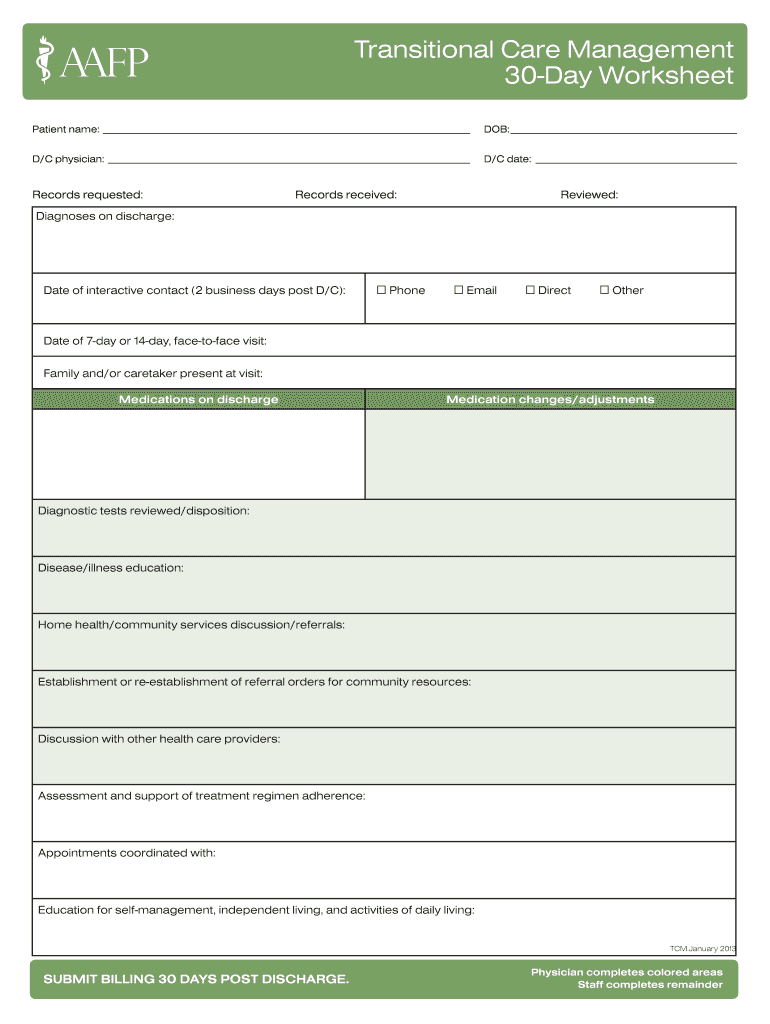
33 Transitional Care Management Worksheet
2 Transitional Care Management Services. AN INTERACTIVE CONTACT. You must make an interactive contact with the beneficiary. and/or caregiver, as appropriate, within 2 business days . following the beneficiary's discharge to the community setting. The contact may be via telephone, e-mail, or face-to-face. Transitional Care Management Worksheet and Human Fetal Derived Enterospheres Provide Insights On Intestinal. Transitional Care Management Worksheet together with A Test Of A Blended Method for Teaching Medical Coding. Transitional Care Management Worksheet or Immaculate Baking organic Chocolate Chip Cookie Mix 15 4 Oz.
transitional period and have started paying medical providers for coordinating Medicare beneficiaries’ care transitions. The new payment plan is intended to acknowledge that effective care transitions require care coordination and provide additional reimbursement to support these activities. Starting in 2013, the physician fee schedule includes

Transitional care management worksheet
Care day worksheet fill online printable fillable blank transitional care management documentation template pdf, The success of any project supervisor depends upon how he utilizes the available resources. For the purpose the job manager should be trained and he needs to be able to meet deadlines. TRANSITIONAL CARE MANAGEMENT SERVICES 2. 3 SUPERVISION The required face-to-face visit must be furnished under a minimum of direct supervision and is subject to applicable State law, scope of practice, and the Medicare Physician Fee. Schedule (PFS) "incident to" rules and regulations. The non-face-to-face services may be Checklist: Transitional Care Management. This checklist is intended to provide healthcare providers with a reference to use when responding to Medical Documentation Requests for Transitional Care Management (TCM) Services. It is not intended to replace published guidelines.
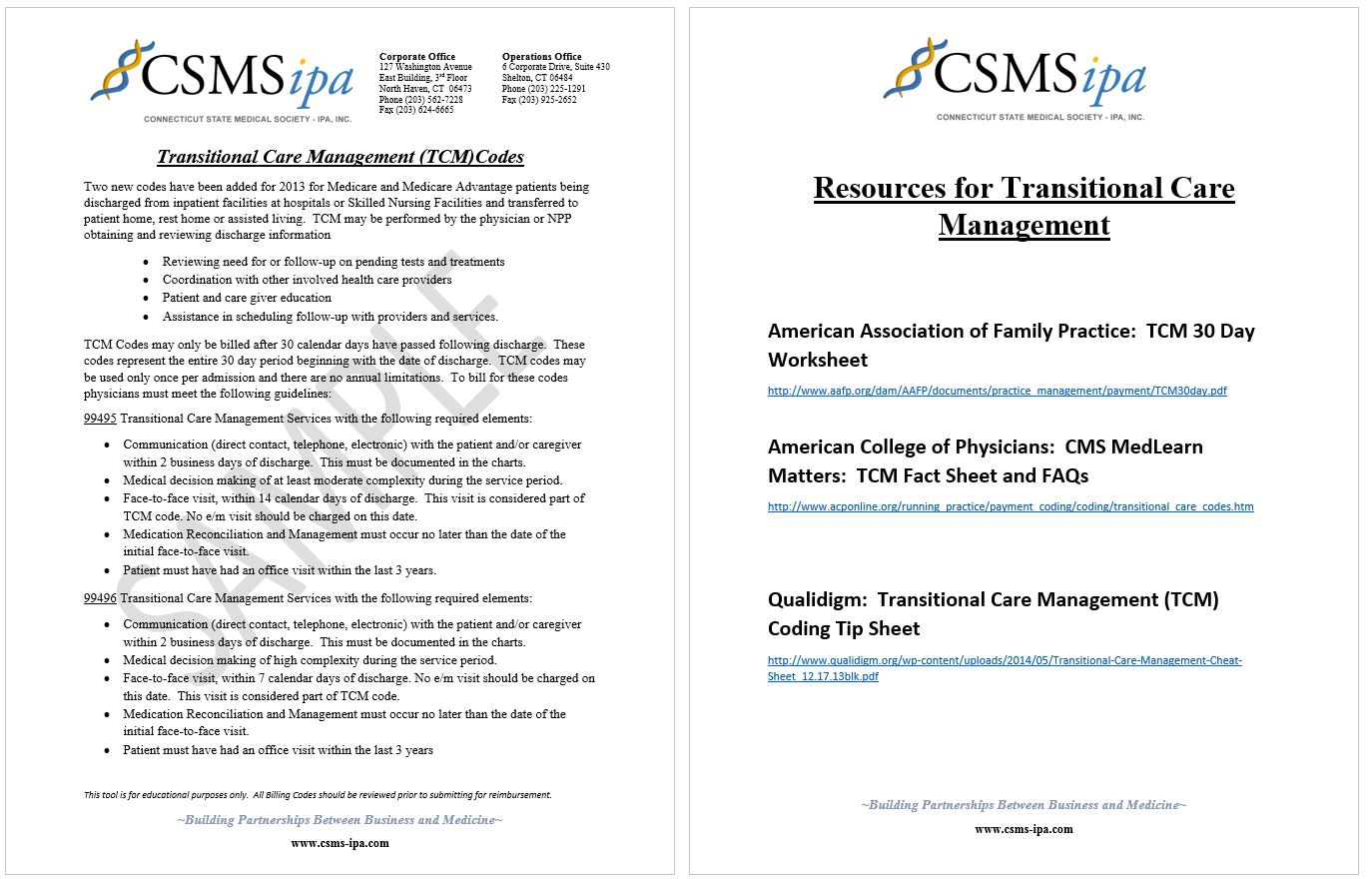
Transitional care management worksheet. primary care and care coordination in improving patient care and reducing healthcare costs. As part of their effort to contain costs, CMS developed the Transitional Care Management (TCM) codes. These codes were designed to reduce 30-day re-hospitalization through reimbursement for care management and care coordination services. CPT - Transitional Care Management Services (99495-99496) Codes 99495 and 99496 are used to report transitional care management services (TCM). These services are for an established patient whose medical and/or psychosocial problems require moderate or high complexity medical decision making This worksheet (ARIES Master Data Collection Form) can be used to remind Medical Case Managers of the. Refer to Nurse Case Management Program for attendant care services. Discuss with client which friends/family can provide client assistance or respite to care giver . ... Refer client to transitional housing programs . Transitional Care Management (As adapted by Confluence Health) Summary of Model: Prior to discharge, hospital staff organize follow-up services and address patients' financial and psychosocial barriers to receiving needed care, drawing on community resources as needed. The bedside RN and inpatient case manager discuss instructions with the patient.
Transitional care management: four common questions. Most family medicine practices manage patients during care transitions, such as from hospital to home, but many practices fail to bill for this. Transitional Care Management. Transitional Care Management Services Fact Sheet (PDF) Related Links. Telehealth; Page Last Modified: 11/17/2021 11:38 AM. Help with File Formats and Plug-Ins. Home. A federal government website managed and paid for by the U.S. Centers for Medicare & Medicaid Services. 7500 Security Boulevard, Baltimore, MD 21244. 99496- Transitional Care Management services with the following required elements: Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge Medical decision making of high complexity during the service period Face-to-face visit, within 7 calendar days of discharge Transition Care Management (TCM) Services (99495-99496) are billed 30 days after dischargefrom a facility, the codes are billedwhen the patient is not present. TCM services are for new or established patients whose medical and/or psychosocial problems require moderate or high complexity medical decision making (MDM) during transitions in care:
transition readiness assessment) with scoring and documentation, per standardized instrument $2.79 NA.08/NA General Behavioral Health Integration Care Management h 99484 Care management services for behavioral health conditions, at least 20 minutes of clinical staff time, directed by a physician or other qualified health 1 TRANSITIONAL CARE ASSIGNMENT WORKSHEET Geriatric Client Objectives: 1. Identify an elderly client in clinical (who is 65 years or older, has poly-pharmacy, dementia or delirium, a fall or fall risk, or end of life care issues) and create a patient centered plan of care focusing on discharge 2. To determine pre-admission functional status 3. To compare current functional status to pre. Transitional Care Management 30-day Worksheet Author: American Academy of Family Physicians Keywords: care management, transitional care, coding, practice management, Created Date: 1/18/2013 3:25:26 PM TRANSITIONAL CARE MANAGEMENT SERVICES 2. 3 SUPERVISION The required face-to-face visit must be furnished under a minimum of direct supervision and is subject to applicable State law, scope of practice, and the Medicare Physician Fee. Schedule (PFS) "incident to" rules and regulations. The non-face-to-face services may be
Free Downloadable Tools Amp Resources Healthcare Training Leader
Model 1: Home Health Model of Care Transitions Work Flow In practice, a home health clinician (a home health nurse, care transition coordinator or coach, or a physical therapist) begins the transitional care at the end of the patient's care in the acute care setting. The clinician will work with the patient prior to discharge following the best
Td Template Job Aid Template 2017 Branding
Care day worksheet fill online printable fillable blank transitional care management documentation template pdf, The success of any project supervisor depends upon how he utilizes the available resources. For the purpose the job manager should be trained and he needs to be able to meet deadlines.
Transitional Care Management
Checklist: Transitional Care Management. This checklist is intended to provide healthcare providers with a reference to use when responding to Medical Documentation Requests for Transitional Care Management (TCM) Services. It is not intended to replace published guidelines.

Transitional Care Management Codes 99495 Cmmi September Ppt
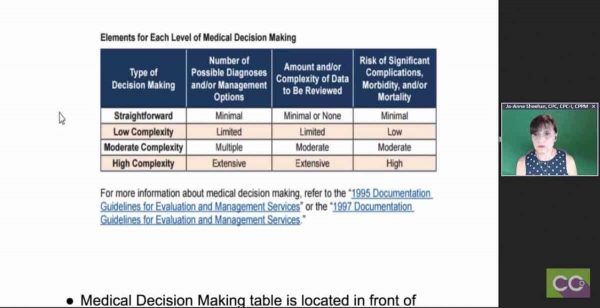
Transitional Care Management (TCM) are services provided to Medicare beneficiaries whose medical and/or psychosocial problems require moderate- or high-complexity medical decision making during.

Transitional Care Management Tcm Mdm Leveling Youtube
Transitional care management (TCM) is intended to reduce potentially preventable readmissions and medical errors during the 30 days following discharge from the acute care setting. The TCM codes recognize the additional work required to provide support to patients after discharge.
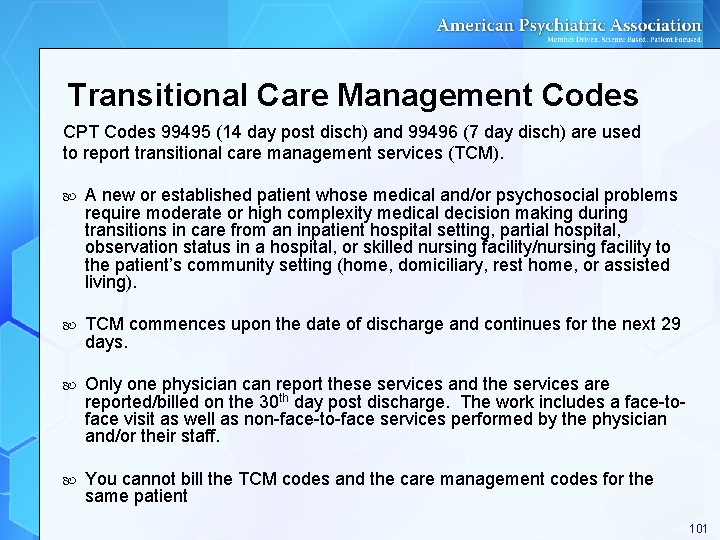
Cpt Coding For Psychiatric Care In 2014 Apa
Transitional Care is complementary, yet not identical to care coordination, disease management, and discharge planning, as transitional care focuses on time-limited services for high-risk vulnerable populations, with an interdisciplinary and education focus (Naylor, et al. (2011). 5. Naylor, Mary. 2008. 6. Naylor, Mary. 2008.
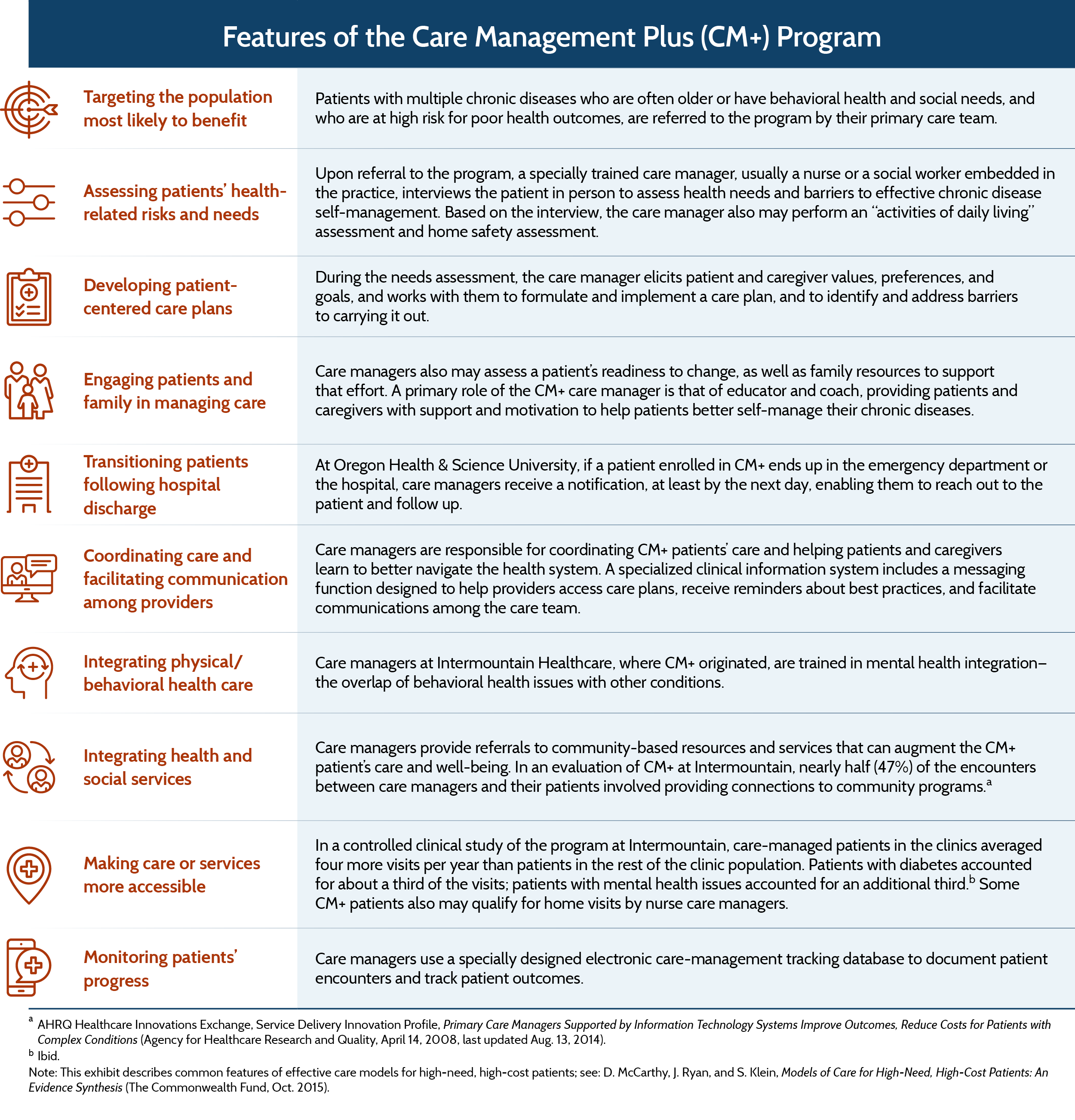
Care Management Plus Strengthening Primary Care For Patients
99495 Transitional Care Management Services with the following required elements: Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge. Medical decision making of at least moderate complexity during the service period. Face-to-face visit, within 14 calendar days of discharge.
The Self Confidence Workbook A Guide To Overcoming Self
Resources about transitional care management (TCM) codes. Access fact sheets, sample documentation and flow sheet, FAQs & other important information.
Payment
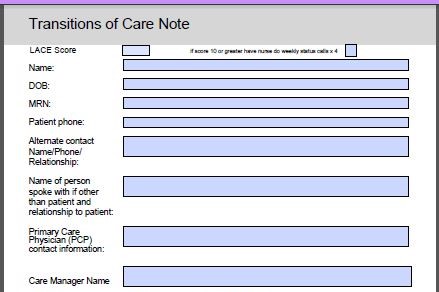
to determine and coordinate the appropriate aspects of individualized care. The goal of case management is to help you manage your health and bring about a better quality of life. As your "case" or care manager, I will be working with you and Dr. _____ to identify your healthcare needs and set up a plan of care that is right for you.
Client Acuity Scale Worksheet
Contact an MCO, ACO, PCMH, health home care manager, as applicable. Contact community clinical, behavioral, and social service providers. Obtain pharmacist consult. Obtain social work consult. Obtain pain management or palliative care consult, as applicable. Obtain psychiatry consult, as applicable. Develop individualized transitional care plan

Review Of Transitional Care Management And Chronic Care
— Transitional Care Management services with the following required elements: Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge; Medical decision making of at least moderate complexity during the

Teacher S Pet 10 Times Tables Activity Worksheet Pack

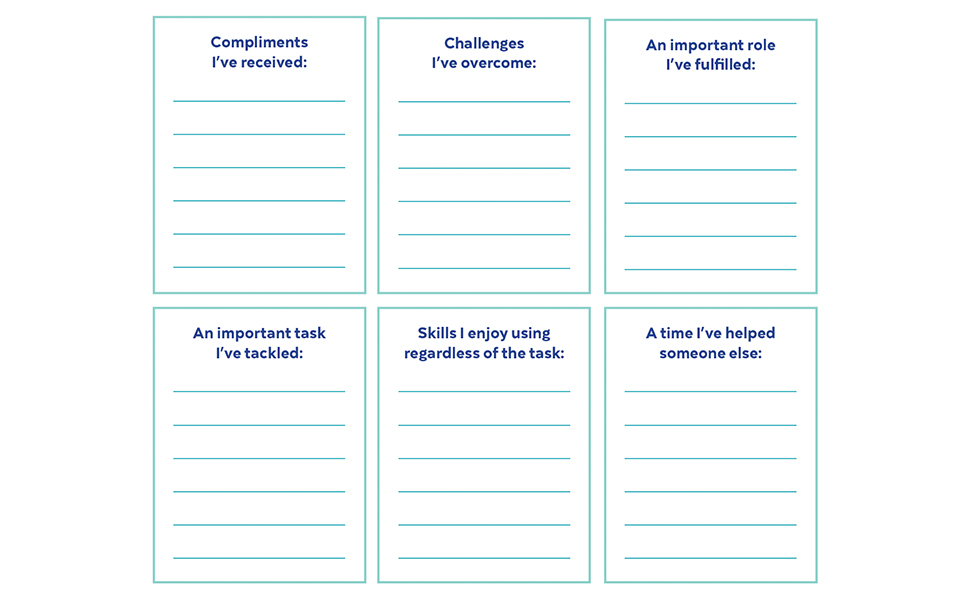
Transition Readiness Program

The Bptrends Process Redesign Methodology Sciencedirect

Transitional Care Management Codes 99495 Cmmi September Ppt
Documentation And Billing For Chronic Care Management

Early Childhood Self Assessment Pasadena Independent School

Mccormick Transitional Care Center Rochester Regional Health

Successes And Challenges In Patient Care Transition
Transitional Care Management Template Fill Online
Coding For Evaluation And Management Services

Clinical Worksheet Henry Williams Part 3 Docx Date Clinical

Essay Writing Worksheets

Quiz Amp Worksheet Vocational Tests For Rehabilitation
Transitional Care Management Tcm Services Mdm Leveling
Transitional Care Management
Federal Register Medicare Program Cy 2020 Revisions To

Readmissions Work Sheet Atom Alliance Case Management
Designing And Delivering Whole Person Transitional Care The
Value Based Practice Resources
Quality Heath Associates Of North Daktoa Sharing Your Success

Jameslhollymd Com Epm Tools Transitions Of Care

Transitional Care Management In The Outpatient Setting Bmj
0 Response to "33 Transitional Care Management Worksheet"
Post a Comment